
Vascularized lymph node transfers (VLNT) surgery is part of Dr. Granzow’s FLOSM comprehensive lymphedema treatment system. Dr. Granzow pioneered the first comprehensive lymphedema treatment system which fully integrates lymphedema surgeries and lymphedema therapy, known as the Functional Lymphatic Operations (FLO)SM System. Dr. Granzow’s treatment system has been consistent and effective in treating lymphedema patients from all over the world.
What makes Dr. Granzow’s lymphedema treatment system unique is his focus on matching the type of lymphedema treatment and surgery to each patient’s condition to produce the maximum effectiveness. The fact is that no single procedure is effective for all cases of lymphedema.
VLNT can be extremely effective for the treatment of lymphedema of the arm or leg. The technique can either replace lymph nodes lost through surgery and/or radiation with healthy, functioning lymph nodes and tissues taken from elsewhere in the body or add lymph nodes to further improve lymphatic drainage.
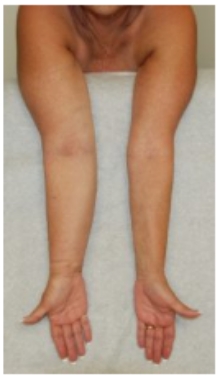
Before Suction Assisted Protein Lipectomy (SAPL)

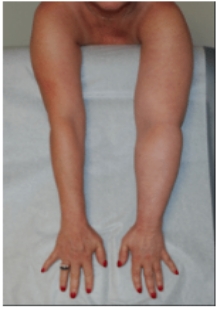
After Suction Assisted Protein Lipectomy (SAPL)
Patient with a prior 17-year history of non-pitting lymphedema of the right arm, treated with SAPL.
After treatment, the affected right arm is now slightly smaller than the unaffected left side.
Patients who have lymphedema swelling in the arm or leg that is not fluid-predominant and has non-pitting edema may be good candidates. In many cases the affected extremity may feel soft, and a careful examination by a trained expert may be required to differentiate soft solid from soft fluid in an arm or leg.

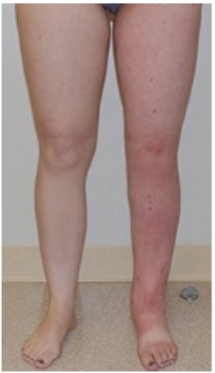
Before Suction Assisted Protein Lipectomy (SAPL)
After Suction Assisted Protein Lipectomy (SAPL)
34 year old patient with a 17-year history of congenital/spontaneous lymphedema of the left leg treated with SAPL. After treatment, the affected left leg is now smaller than the unaffected right leg.
The SAPL surgery has been proven to be safe and has consistent results both in our experience and in research published in multiple prominent medical journals. The lymphatics in the arm or leg are not damaged by the surgery. In fact, the reduction of excess fats and other solids improve the lymphatic drainage of the limb and considerably improve the management of the affected areas.
Massive obesity on its own has been shown to cause lymphedema, and multiple theories exist to explain the decreased lymphatic function in severely overweight arms and legs. Significantly overweight patients are not appropriate surgical candidates for lymphedema surgery. However, weight loss itself has been shown to improve such lymphedema.
It is critical to note that SAPL is different from cosmetic liposuction techniques, and this technique should not be performed by surgeons who are not specifically trained in this specialized type of procedure. A team approach with an experienced surgeon and trained lymphedema therapist is required.


Dr. Granzow in surgery with Dr. Hakan Brorson in Malmo, Sweden
This specialized liposuction has been shown to be effective in reducing the size and firmness of the affected arm or leg for more than 20 years. Our results are consistent with those in the published literature.
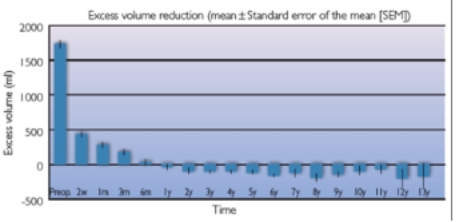
Mean postoperative excess volume reduction in 95 women with arm lymphedema following breast cancer, from Brorson, The Facts About Liposuction As A Treatment For Lymphoedema, Journal of Lymphoedema, 2008
The volume reductions achieved are permanent with continued compression following SAPL surgery. Dr. Granzow now offers additional surgeries, such as a Vascularized Lymph Node Transfer (VLNT) and/or Lymphaticovenous Anastomosis (LVA), at a later time to reduce the amount of compression needed to maintain the volume reduction. Dr. Granzow’s method of combining lymphedema surgeries has shown excellent results. He was the first surgeon to successfully perform SAPL with subsequent VLNT and also LVA surgeries for the same patient to reduce the requirement for postoperative sleeve use.

Patient Before Lymphedema Surgeries
Patient After Lymphedema Surgeries
Patient 18 Months After Lymphatic Liposuction and 7 Months After Vascularized Lymph Node Transfer.
A volume reduction of over 80% was achieved and a compression garment is no longer worn during the day.
Dr. Granzow has found that the removal of pathologic lymphedema solids and fat with the SAPL procedure typically has improved the lymphatic drainage of an
affected arm or leg. Peer-reviewed papers in the medical literature have shown that SAPL has been shown to significantly decrease the incidence of surgical
infections and cellulitis after surgery. Studies specifically looking at the lymphatic system before and after SAPL also have shown that SAPL does not appear to
further damage the already damaged lymphatics in an arm or leg affected by lymphedema.
For any kind of quarries or information's feel free to contact us